
What Happens When a Basement Flood Sits for 48 Hours
Most people think water damage is about how much water came in. It’s not. It’s about how long...
Read MoreMost people think water damage is about how much water came in. It’s not. It’s about how long...
Read More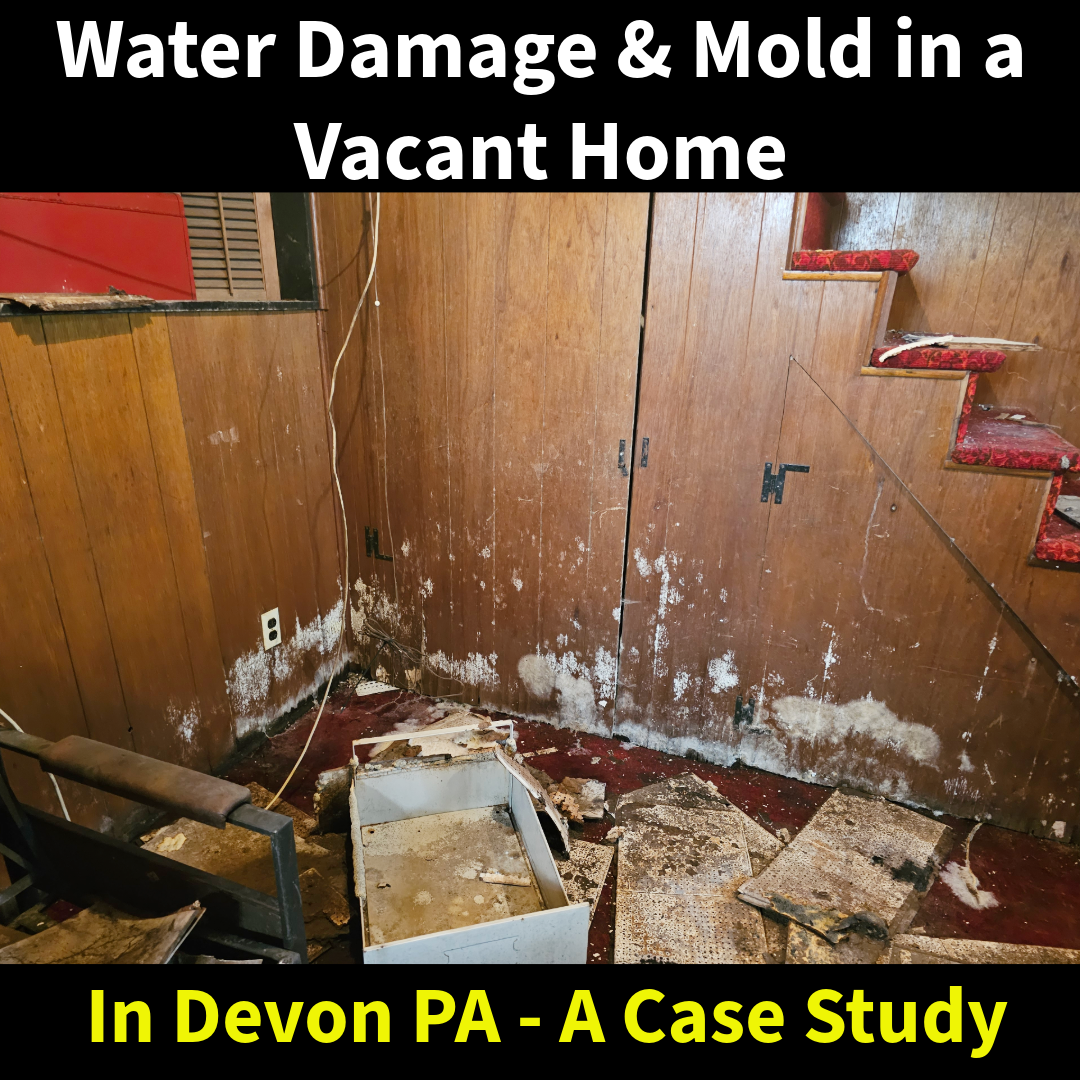
Not all water damage happens in an occupied home. In some cases, the worst situations are the ones...
Read More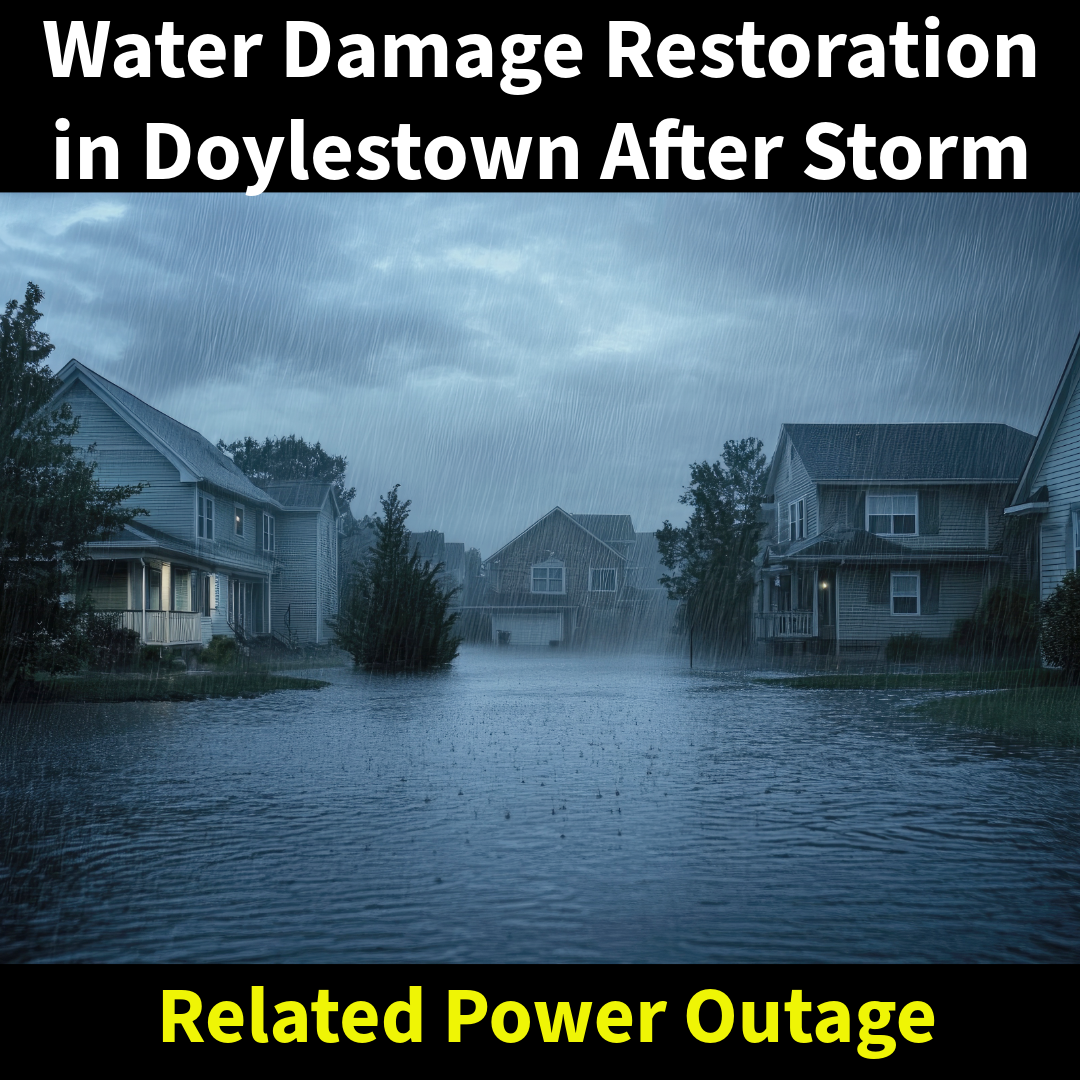
Severe storms moved through Doylestown this past Saturday night, knocking down multiple trees and causing widespread power outages....
Read More
Most people think fireworks start fires when they land on a roof or explode near a home. An...
Read More
Spraying mold is one of the most common shortcuts in this industry. It may change the way a...
Read More
Water damage is not just about removing visible water. The real issue is what remains behind. When materials...
Read More